
Diagnostic
Clinique & ECG
– Douleur angineuse continue et récente (plus de 15 minutes)
– ECG :
- Sus décalage de ST dans 2 dérivations adjacentes > 0.1mV dans les standards > 0.2mV dans les précordiales
- images en miroir
- Sous décalage de ST dans 2 dérivations adjacentes
- ECG normal
– douleur trinitro-résistante
consultez le simulateur ECG

Importance de l’anamnèse
– ATCD personnels, terrain, facteurs de risque cardiovasculaire, circonstances de survenue
– Rechercher un diabète, une insuffisance rénale (facteurs de gravité).
Diagnostics différentiels
– péricardite, myocardite, dissection aortique, embolie pulmonaire, intoxication digitalique, intoxication au CO...
BILAN PARACLINIQUE
Bilan de routine
– ECG 18 dérivations (à renouveler)
– Glycémie capillaire
– Monitorage Scope, PNI, SpO2
Bilan spécifique
– Hémostase (Groupe, NFS, plaquettes, TP, TCA)
– Myoglobine + Troponine (en cas de ST+ ne pas attendre les résultats pour entreprendre la recanalisation d’urgence).
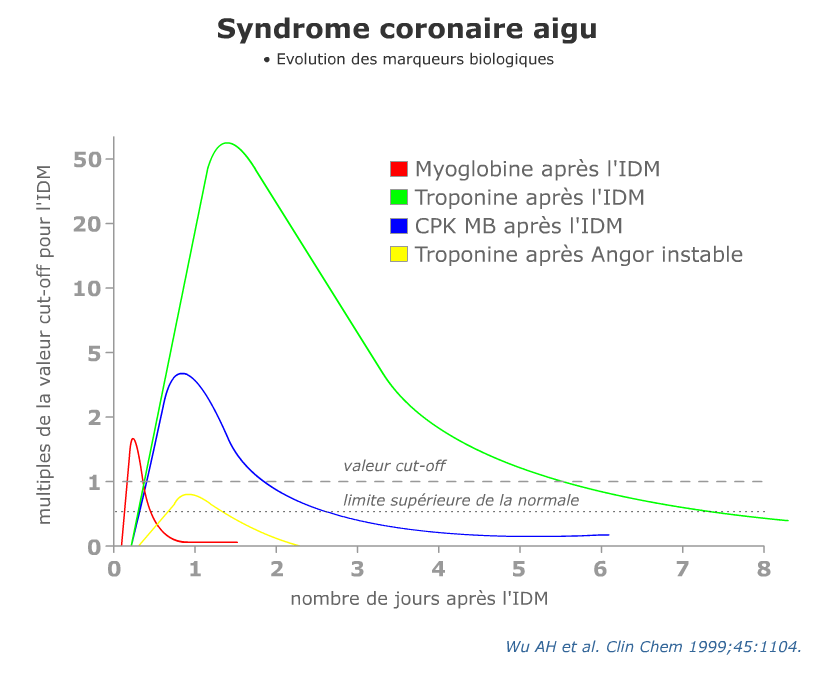
La troponine s’élève entre la quatrième et la sixième heure. Répéter le prélèvement +++
Interprétation des résultats de la Troponine T ultra sensible
– TnTc HS <0,014 ng/mL :
- et douleur thoracique > 3h
- sortie avec discussion des explorations ambulatoires à 30 jours
- et douleur thoracique < 3h
- répéter le dosage 3 heures après le premier prélèvement
- augmentation <0,007 ng/mL ou <30%, sortie avec discussion des explorations ambulatoires à 30 jours
- augmentation >0,007 ng/mL ou >30%, discuter avec le cardiologue de l’admission pour explorations.
- répéter le dosage 3 heures après le premier prélèvement
– TnTc HS 0,014-0,05 ng/L :
- répéter le dosage 3 heures après le premier prélèvement
- augmentation <0,007 ng/mL ou <30%, sortie avec discussion des explorations ambulatoires à 30 jours
- augmentation >0,007 ng/mL ou >30%, discuter avec le cardiologue de l’admission pour explorations.
– TnTc HS >0,05 ng/mL :
- discuter avec le cardiologue de l’admission pour explorations.
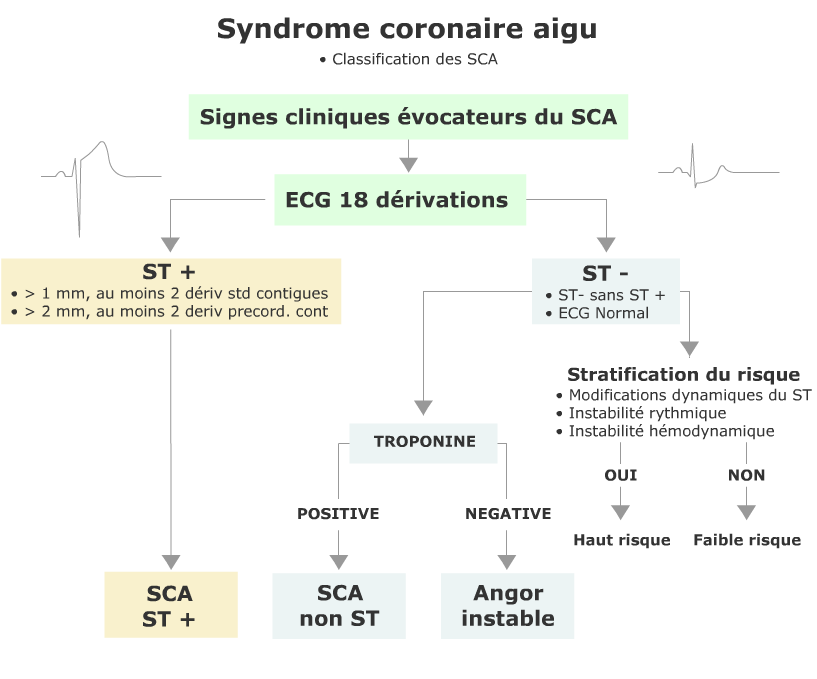
Classification des SCA
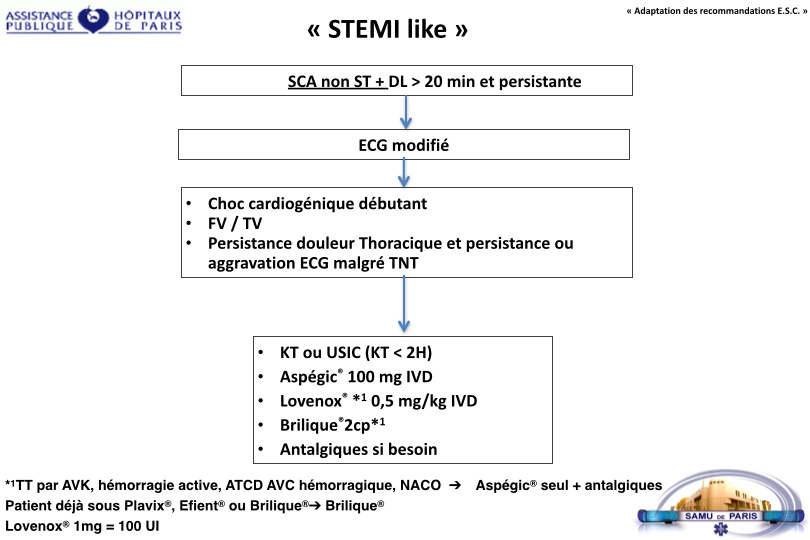
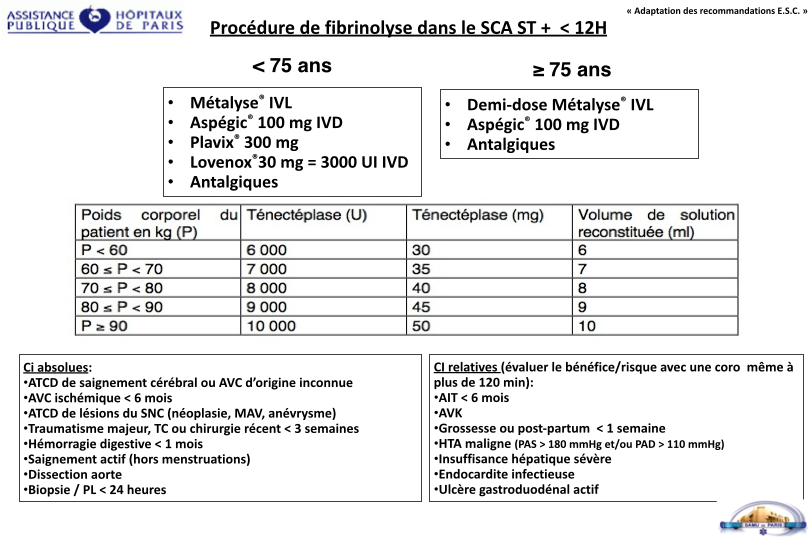
TRAITEMENT
Thérapeutique symptomatique
– Test aux dérivés nitrés. L’usage intra veineux est limité aux SCA non ST (en respectant les contre indications) et en surveillant étroitement la PA la fonction ventriculaire droite.
– Morphine titrée (en fonction de l’EVS) , anxiolytiques éventuels.
– 2 voies veineuses (G5% et Nacl) en garde veine.
– O2 si spo2 < 93% ou Killip > 1
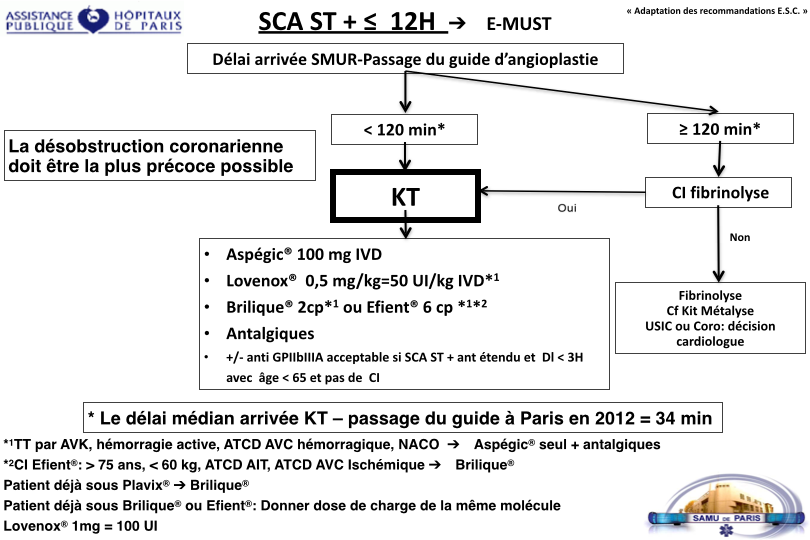
Thérapeutique spécifique
Protocole officiel du SAMU de PARIS, SMUR Necker, SMUR Hôtel Dieu, SMUR Lariboisiere, SMUR Pitié.


Rappels de pharmacologie :
| Nom | Classe | Action | Administration |
|---|---|---|---|
| Clopidogrel (Plavix®) | anti-adhésif et anti-agrégant plaquettaire de la classe des thiénopyridines antagoniste irréversible du récepteur P2Y à l’ADP, ce qui empêche l’activation du complexe GPIIb-IIIa. |
Délai d’action : 2h Pic : 6h Durée d’action : 7-10 jours (durée de vie des plaquettes) |
per os |
| Ticagrelor (Brilique®) | anti-adhésif et anti-agrégant plaquettaire de la classe des cyclopentyltriazolopyrimidines antagoniste sélectif et réversible du P2Y, n’agissant pas au site d’action de l’ADP, mais empêchant la transduction du signal. |
Délai d’action : < 30 min Pic : 2-4h Durée d’action : 4 jours |
per os |
| Prasugrel (Efient®) | anti-adhésif et anti-agrégant plaquettaire de la classe des thiénopyridines antagoniste irréversible du récepteur P2Y à l’ADP, ce qui empêche l’activation du complexe GPIIb-IIIa. |
Délai d’action : < 30 min Pic : 4h Durée d’action : 7-10 jours (durée de vie des plaquettes) |
per os |

TIMI Score Risk pour le SCA non ST
| --- Facteur de risque --- | --- Points --- | --- Mortalité à J 14 --- |
|---|---|---|
| à‚ge >= 65 ans | 1 | 5% |
| > 3 facteurs de risque coronaire | 1 | 8% |
| Cardiopathie ischémique reconnue | 1 | 13% |
| prise d’aspirine au cours des 7 derniers jours | 1 | 20% |
| Douleur angineuse récente | 1 | 26% |
| Augmentation des enzymes | 1 | 41% |
| Sous décalage de ST > 0,5 mm | 1 | - |
Score de risque = Total des points (0-7)
– Classification ESC
| Patient à haut risque | Patients à faible risque |
|---|---|
| douleurs thoraciques récidivantes et/ou modifications dynamiques du ST | pas de douleur thoracique au cours de la période d’observation |
| modifications du segment ST non interprétables | ST normal mais T<0 ou plates |
| élévation du taux de troponine | |
| troponine normale | |
| instabilité hémodynamique | |
| arythmies majeures TV/FV | |
| diabète type 1 | |
| angor instable précoce après IDM |
– Calculateurs de risque
Références
– Acute coronary syndromes, Scottish Intercollegiate Guidelines Network - SIGN (Feb 2013)
– Steg G, James S et al. ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation European Heart Journal (2012) 33, 2569&2619
– Scheuermeyer FX, Innes G, Grafstein E, et al. Safety and Efficiency of a Chest Pain Diagnostic Algorithm With Selective Outpatient Stress Testing for Emergency Department Patients With Potential Ischemic Chest Pain. Ann Emerg Med. Jan 4 2012 ;
– Hamm CW, Bassand JP, Agewall S, et al. ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation : The Task Force for the management of acute coronary syndromes (ACS) in patients presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. Sep 21 2011
– Hyperglycaemia in acute coronary syndromes, NICE Clinical Guideline (October 2011)
– Acute coronary syndromes - ticagrelor, NICE Technology Appraisal Guideline (October 2011)
– Heidenreich PA, Alloggiamento T, Melsop K, McDonald KM, Go AS, Hlatky MA. The prognostic value of troponin in patients with non-ST elevation acute coronary syndromes : a meta-analysis. J Am Coll Cardiol. Aug 2001 ;38(2):478-85.
– O’Connor RE, Bossaert L, Arntz HR, Brooks SC, Diercks D, Feitosa-Filho G, et al. Part 9 : acute coronary syndromes : 2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation. Oct 19 2010 ;122(16 Suppl 2):S422-65.
– Heidenreich PA, Alloggiamento T, Melsop K, McDonald KM, Go AS, Hlatky MA. The prognostic value of troponin in patients with non-ST elevation acute coronary syndromes : a meta-analysis. J Am Coll Cardiol. Aug 2001 ;38(2):478-85.
– Chest pain of recent onset, NICE Clinical Guideline (March 2010)
– Unstable angina and NSTEMI, NICE Clinical Guideline (March 2010)
– Swanson N, Montalescot G, Eagle KA, et al ; Delay to angiography and outcomes following presentation with high-risk, Heart. 2009 Mar ;95(3):211-5. Epub 2008 Sep 18.
– Acute coronary syndrome - prasugrel, NICE Technology Appraisal Guideline (October 2009)
– Peters RJ, Mehta S, Yusuf S ; Acute coronary syndromes without ST segment elevation. BMJ. 2007 Jun 16 ;334(7606):1265-9.
– Cohen M, Diez JE, Levine GN, et al ; Pharmacoinvasive management of acute coronary syndrome : incorporating the 2007 ACC/AHA guidelines : the CATH (cardiac catheterization and antithrombotic therapy in the hospital) Clinical Consensus Panel Report—III. J Invasive Cardiol. 2007 Dec ;19(12):525-38 ; quiz 539-40.
– Conway Morris A, Caesar D, Gray S, et al ; TIMI risk score accurately risk stratifies patients with undifferentiated chest pain presenting to an emergency department. Heart. 2006 Sep ;92(9):1333-4.
– Sabatine MS, Morrow DA, Giugliano RP, et al ; Implications of upstream glycoprotein IIb/IIIa inhibition and coronary artery stenting in the invasive management of unstable angina/non-ST-elevation myocardial infarction : a comparison of the Thrombolysis In Myocardial Infarction (TIMI) IIIB trial and the Treat angina with Aggrastat and determine Cost of Therapy with Invasive or Conservative Strategy (TACTICS)-TIMI 18 trial. Circulation. 2004 Feb 24 ;109(7):874-80. Epub 2004 Feb 2.
– Lagerqvist B, Husted S, Kontny F, et al ; A long-term perspective on the protective effects of an early invasive strategy in unstable coronary artery disease : two-year follow-up of the FRISC-II invasive study. J Am Coll Cardiol. 2002 Dec 4 ;40(11):1902-14.
– Culic V, Eterovic D, Miric D, et al ; Symptom presentation of acute myocardial infarction : influence of sex, age, and risk factors. Am Heart J. 2002 Dec ;144(6):1012-7.
– Alpert JS, Thygesen K, Antman E, Bassand JP. Myocardial infarction redefined—a consensus document of The Joint European Society of Cardiology/American College of Cardiology Committee for the redefinition of myocardial infarction. J Am Coll Cardiol. Sep 2000 ;36(3):959-69.
– Antman EM, Tanasijevic MJ, Thompson B, Schactman M, McCabe CH, Cannon CP, et al. Cardiac-specific troponin I levels to predict the risk of mortality in patients with acute coronary syndromes. N Engl J Med. Oct 31 1996 ;335(18):1342-9.
– Heidenreich PA, Alloggiamento T, Melsop K, McDonald KM, Go AS, Hlatky MA. The prognostic value of troponin in patients with non-ST elevation acute coronary syndromes : a meta-analysis. J Am Coll Cardiol. Aug 2001 ;38(2):478-85.
– GRACE ; Global Registry of Acute Cardiac Events
– The TIMI Study Group

